Two phrases that sound similar but mean different things clinically — and the confusion between them leads many women to misinterpret their fertility results entirely. At Dr. Aravind's IVF Fertility and Pregnancy Centre, the best fertility hospital in Chennai, clarifying this distinction is one of the most important conversations that happens in the first consultation.
Here is what each actually means, why they are related but not identical, and what the difference means for your treatment options.
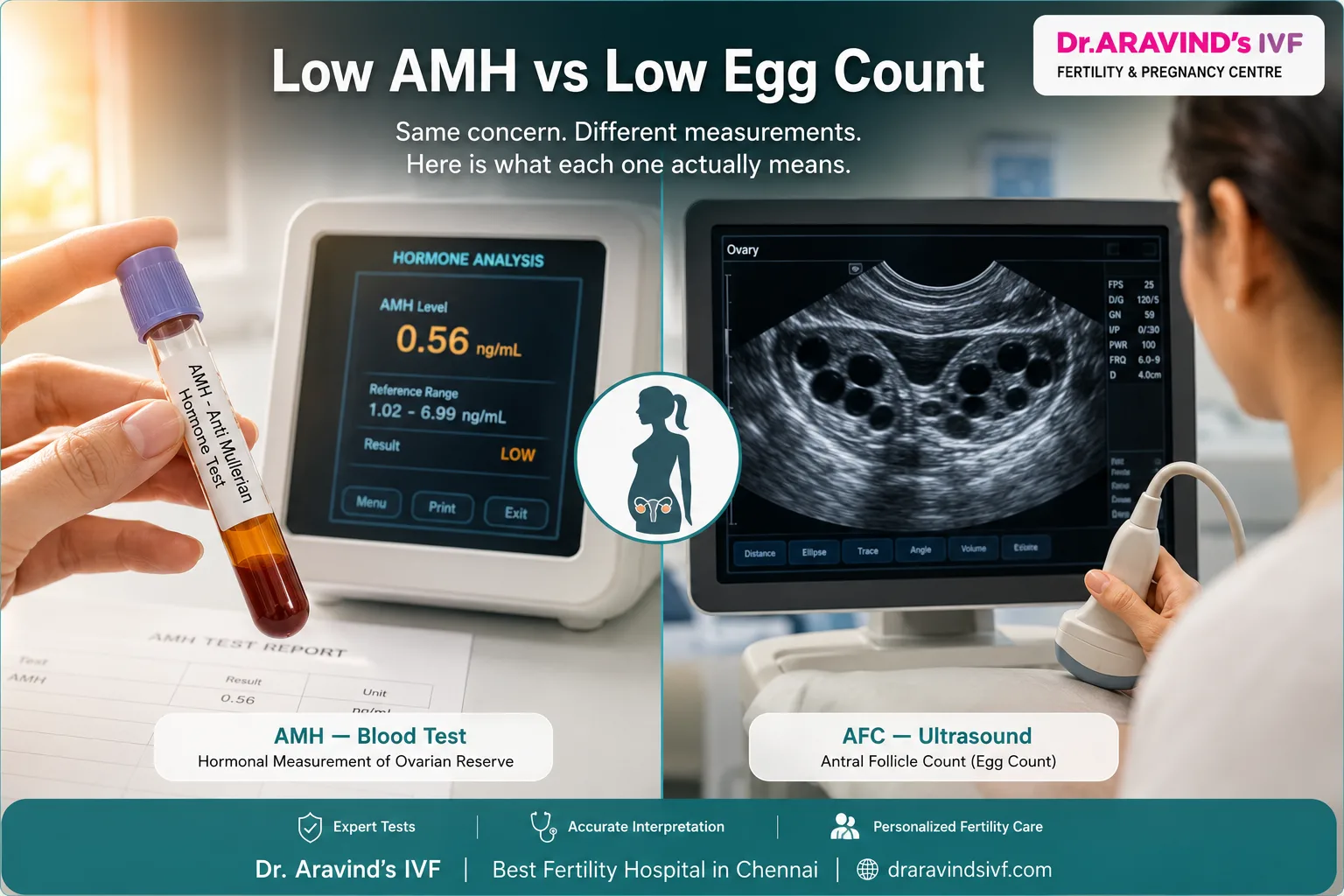
What Is AMH?
AMH — Anti-Mullerian Hormone — is a hormone produced by the small developing follicles in the ovaries. It is measured through a blood test and used as a clinical marker of ovarian reserve.
- AMH reflects the number of small antral follicles currently active in the ovaries
- It is a hormonal measurement — an indirect indicator of egg supply
- It can be tested on any day of the menstrual cycle without timing constraints
- A low AMH result indicates that fewer follicles are producing this hormone — suggesting a smaller egg pool
Low AMH means the hormone level is below the expected range for the patient's age.
What Is Low Egg Count?
Low egg count — more precisely called diminished ovarian reserve — refers to the actual number of eggs remaining in the ovaries being below what is expected for age.
- It is assessed most directly through antral follicle count (AFC) via transvaginal ultrasound
- AFC counts the number of small visible follicles across both ovaries on Day 2 or Day 3 of the cycle
- A count below 5 to 7 follicles across both ovaries is considered low
- Low egg count can also be inferred from elevated Day 3 FSH — the pituitary working harder to stimulate a depleted reserve
Low egg count is the physical reality. AMH is one of the hormonal markers used to estimate it.
How AMH and Egg Count Relate — and Where They Diverge
- Low AMH and low egg count are closely correlated — they usually appear together
- But they are not always identical measurements of the same thing
- A woman can have low AMH with a relatively normal AFC — or vice versa
- AMH can be temporarily suppressed by factors including oral contraceptive use, vitamin D deficiency, and certain medications
- AFC gives a more direct visual picture of the follicle pool at that specific moment in the cycle
This is why the best fertility hospital in Chennai never diagnoses diminished ovarian reserve from AMH alone. Both AMH and AFC together — alongside Day 3 FSH and estradiol — form the complete ovarian reserve assessment.
Why the Distinction Matters for Treatment
Understanding whether you have low AMH, low egg count, or both directly shapes what treatment approach is most appropriate.
Low AMH with normal AFC:
- May indicate temporary hormonal suppression
- Stimulation response may be better than the AMH number alone predicts
- Repeat testing after stopping oral contraceptives often produces a different result
Low AFC with low AMH:
- Confirms diminished ovarian reserve from both hormonal and ultrasound evidence
- Stimulation protocols are adjusted to maximise recruitment from a genuinely smaller pool
- PGT-A chromosomal screening becomes more clinically relevant when embryo numbers are limited
Elevated FSH alongside both:
- Confirms the pituitary is compensating for reduced ovarian response
- More aggressive stimulation may be required to achieve adequate follicle recruitment
At the best IVF centre in India, treatment planning for diminished ovarian reserve uses all three markers together — never one in isolation.
What Low Numbers Do Not Tell You
Both low AMH and low egg count measure quantity — not quality.
- Egg quality is determined primarily by age
- A 31-year-old with low AMH has 31-year-old eggs — chromosomally healthier than the eggs of a 40-year-old with normal AMH
- Many women with both low AMH and low AFC achieve successful pregnancies through IVF with appropriately tailored protocols
- The number on the report is context — not conclusion
The Practical Takeaway
- Low AMH and low egg count are related but distinct measurements
- Both should be assessed together — never interpreted in isolation
- Neither is a definitive barrier to pregnancy
- What matters is the complete clinical picture — age, AMH, AFC, FSH, and full hormonal profile together
Dr. Aravind's IVF Fertility and Pregnancy Centre builds every ovarian reserve assessment around this complete picture — so that treatment recommendations are based on the whole story, not a single number.
📍 Dr. Aravind's IVF Fertility and Pregnancy Centre, Chennai
📞 +91 90 2012 2012
🔗 https://www.draravindsivf.com/chennai/chennai-detail