Peyronie’s disease is a chronic condition involving the development of fibrous scar tissue (plaques) within the penis, leading to abnormal curvature, deformity, pain, and in many cases, sexual dysfunction. While often misunderstood or ignored due to stigma, this condition has a well-documented medical basis and a growing range of effective treatments.
This comprehensive guide explores the condition at a deeper clinical level—covering anatomy, pathology, progression, and modern treatment approaches.
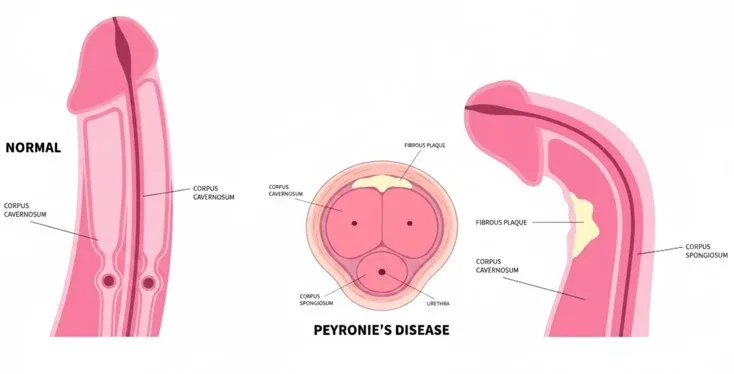
Penile Anatomy and the Mechanism of Curvature
The penis is composed of three main structures:
- Two corpora cavernosa (erectile chambers responsible for rigidity)
- One corpus spongiosum (surrounds the urethra)
These structures are encased in a tough, elastic fibrous layer called the tunica albuginea.
Normal Erection Process
- Blood fills the corpora cavernosa
- Tunica albuginea stretches symmetrically
- Result: a straight erection
In Peyronie’s Disease
- Scar tissue forms in localized areas
- These areas cannot expand normally
- Result: uneven expansion → penile curvature toward the affected side
Pathophysiology: What Happens at the Cellular Level?
Peyronie’s disease is essentially a disorder of abnormal wound healing.
Key Processes Involved:
- Microvascular Injury
- Repeated minor trauma damages small blood vessels
- Inflammatory Response
- Immune cells release cytokines and growth factors
- Fibrosis Formation
- Overproduction of collagen (especially Type I and III)
- Reduced collagen breakdown
- Plaque Development
- Dense, fibrotic tissue replaces normal elastic tissue
- In some cases, plaques become calcified
Risk Factors (Expanded Clinical View)
Several medical and lifestyle factors increase susceptibility:
1. Age
- Most common in men aged 40–70
- Reduced regenerative capacity of tissues
2. Genetic Links
- Strong association with:
- Dupuytren’s contracture
- Family history of fibrotic disorders
3. Metabolic Diseases
- Diabetes mellitus
- Dyslipidemia
4. Vascular Disorders
- Hypertension
- Atherosclerosis
5. Lifestyle Factors
- Smoking (impairs blood flow and healing)
- Alcohol (indirect effects on vascular health)
Clinical Presentation: Beyond Basic Symptoms
1. Penile Curvature (Primary Feature)
- Can range from mild (<20°) to severe (>90°)
- Direction depends on plaque location:
- Dorsal plaque → upward curvature
- Ventral plaque → downward curvature
- Lateral plaque → sideways bending
2. Plaque Characteristics
- Firm, well-defined areas
- May feel:
- Flat
- Nodular
- Cord-like
3. Pain Patterns
- Common in early inflammatory stage
- Typically resolves in chronic phase
4. Erectile Dysfunction
Erectile dysfunction occurs in up to 30–50% of patients due to:
- Vascular insufficiency
- Venous leak
- Psychological inhibition
5. Complex Deformities
Advanced disease may present with:
- Hourglass deformity
- Penile indentation
- Hinge effect (instability during erection)
6. Penile Shortening
Occurs due to:
- Loss of elasticity
- Surgical interventions (in some cases)
Disease Progression: Acute vs Chronic Phase
Acute Phase (Active Phase)
- Duration: 6–18 months
- Ongoing inflammation
- Progressive curvature
- Pain during erection
Chronic Phase (Stable Phase)
- No further worsening
- Pain subsides
- Plaques stabilize or calcify
Diagnostic Evaluation (Advanced Approach)
1. Physical Examination
- Palpation of plaques
- Measurement of penile length
2. Imaging Modalities
Penile Ultrasound (Gold Standard)
- Detects:
- Plaque size
- Calcification
- Blood flow abnormalities
Doppler Ultrasound
- Evaluates vascular integrity
- Identifies arterial insufficiency or venous leak
3. Induced Erection Test
- Intracavernosal injection used
- Allows accurate measurement of:
- Curvature angle
- Deformity type
Treatment: Evidence-Based Management
Treatment depends on:
- Stage of disease
- Severity
- Erectile function
- Patient expectations
Non-Surgical Management (First-Line)
1. Intralesional Therapy (Most Effective Non-Surgical Option)
Collagenase Injections
- Break down collagen in plaques
- Improve curvature significantly
Protocol:
- Multiple cycles
- Combined with modeling techniques
2. Oral Therapies (Limited Evidence)
- Vitamin E
- Tamoxifen
- Potaba
These are less effective but sometimes used adjunctively.
3. Mechanical Therapy
Penile Traction Devices
- Gradual stretching
- Reduces curvature
- Improves length
Vacuum Devices
- Enhance blood flow
- Maintain penile structure
4. Shockwave Therapy
- Primarily reduces pain
- Minimal effect on curvature
Surgical Treatment (Definitive Management)
Indicated when:
- Curvature prevents intercourse
- Disease is stable (≥6 months)
1. Tunica Plication
- Shortens the longer side
- Straightens penis
Advantages:
- High success rate
- Low complication risk
Disadvantages:
- Penile shortening
2. Plaque Incision with Grafting
- Plaque is incised or removed
- Graft inserted
Advantages:
- Preserves length
Risks:
- Erectile dysfunction
- Longer recovery
3. Penile Prosthesis (Implants)
Penile implant surgery is used when:
- Severe curvature + ED coexist
Benefits:
- Restores rigidity
- Corrects deformity
Complications and Long-Term Effects
Untreated Peyronie’s disease can result in:
- Severe penile deformity
- Chronic erectile dysfunction
- Painful intercourse
- Psychological distress
- Relationship difficulties
Psychological Impact (Often Overlooked)
Mental health effects can be significant:
- Performance anxiety
- Depression
- Avoidance of intimacy
Psychological counseling is often recommended alongside medical treatment.
Lifestyle Modifications (Supportive Care)
- Stop smoking
- Control diabetes and hypertension
- Avoid penile trauma
- Maintain a balanced diet
- Regular exercise
Prognosis
- Mild cases: may stabilize or improve
- Moderate cases: require medical therapy
- Severe cases: often need surgery
Early treatment leads to better outcomes and less deformity.
When to Seek Medical Help
Consult a urologist if you experience:
- New penile curvature
- Pain during erection
- Noticeable lumps
- Difficulty with intercourse
Final Conclusion
Peyronie’s disease is a medically recognized condition with a clear biological basis—not something to ignore or feel embarrassed about.
With modern advancements in diagnosis and treatment, most patients can achieve significant improvement or complete functional recovery.


