What is a PDX Model and How to Make a PDX Model?
Cancer is a major threat to human life and health globally and is second only to cardiovascular disease in terms of morbidity and mortality. Cancer remains a focus of attention of health services worldwide. Good animal models can not only be used to study the occurrence, development, and biological mechanisms of cancer but also to screen anti-cancer drugs and gene therapies. In recent years, patient-derived xenograft(PDX) models have become a research hotspot due to their ability to preserve the microenvironment and histological characteristics of primary tumors. This review summarizes the method of PDX animal modeling and its application in oncology medicine, as well as its limitations, providing an important reference for the application of PDX models in the field of tumor therapy.[1]
What is a PDX mouse model and what is PDX vs CDX model?
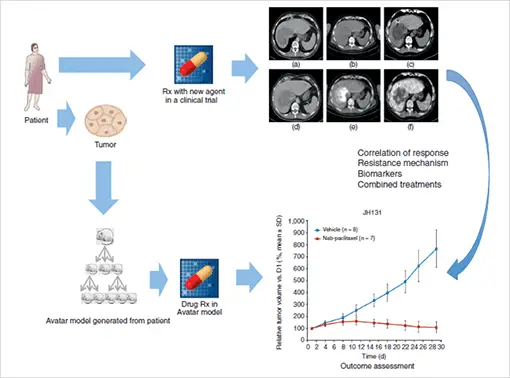
In the PDX model, small tumors surgically excised from cancer patients are implanted into highly immunodeficient mice, allowing the tumors to grow and then transplanted into secondary recipient mice. Compared with the CDX model, the PDX model transplants intact tumor tissue into the recipient animal with the tumor structure and the relative proportion of cancer cells and stromal cells kept unchanged, resulting in enhanced consistency with human disease. [2] The patient-derived xenograft (PDX) model retains the cell morphology, tissue structure characteristics, and genetic characteristics similar to the patient to the greatest extent of the original tumor. The PDX model provides a new platform for studying the response of cancer patients to radiotherapy and chemotherapy, seeking new therapeutic targets, and improving prognosis, bringing personalized precision therapy research into a new stage.
Features and benefits of PDX models
Features of PDX models
PDX models are an important in-vivo platform for studying tumor development, drug response mechanisms, and personalized patient therapies. The first-generation PDX model (Po) was obtained by implanting human tumor tissues or cells into immunodeficient mice and then passing Po’s tumor tissues or cells into multiple new immunodeficient mice (P1), After repeated passages, we can establish tumor-bearing mice that can stably retain the morphological, molecular biological, and genetic characteristics of the patient’s initial tumor. During transplantation and passaging, human cells and tumor cells are preserved, while stromal cells are replaced by mouse cells, which is a defining feature of PDX models.
Advantages of PDX Models
One of the main advantages of PDX models in tumor research is that they preserve the cell morphology and tissue structure characteristics of the original tumor to the greatest extent. The tumor microenvironment includes extracellular matrix (ECM) and stromal cells, which in turn include endothelial cells, pericytes, immune cells, cancer-associated fibroblasts (CAF), and pro-inflammatory cells.
Since the PDX model retains the heterogeneity of the tumor, compared with other experimental animal models, the PDX model can better predict the occurrence and development of tumors in the human body and the response of tumor patients to treatment, helping to distinguish the most suitable treatment for patients, find therapeutic targets, and then carry out personalized and precise treatment for patients. PDX models can also be used to identify patients with tumors resistant to chemotherapy and to determine the relationship between drug resistance and genetic mutations. [3]
Development history of the PDX model
As early as 1969, the Danish scientist Rygaard et al. successfully transplanted human colon tumor tissue into nude mice with hypoplastic thymus for the first time, which was the earliest attempt at xenotransplantation. However, the limited success rate of PDX modeling has severely hindered its development. Until 1992, the Jackson Laboratory of the United States bred nonobese diabetic/severe combined immunodeficient (NOD/SCID) mice with T, B, and NK cell defects so that the PDX model of hematological tumors could be stably constructed, and it was also the PDX model for solid tumors. In 2006, Rubio-Viqueira of Johns Hopkins University successfully established the PDX model through NOD/SCID mice. The team has significantly advanced the PDX development process by improving the modeling success rate. At the same time, a series of problems with the NCI60 cell line has also been widely recognized by researchers around the world. As a result, PDX models became popular in the early 2000s. In 2014, the PDX model was on the cover of Science magazine because of its close connection with clinical practice. In recent years, some research institutes and drug companies are scrambling to develop PDX models. PDX models are considered to be perfect models for evaluating anticancer drugs.
Selection of PDX model immunodeficient mice
Currently, PDX immunodeficiency mouse strains mainly include four types: nude mice lacking functional T cells (Nude mice); severe combined immunodeficiency mice lacking functional T cells and B cells (Severe combined immunodeficiency mice, SCID); nonobese diabetic/severe combined immunodeficiency mice lacking functional T and B cells and impaired NK cells (NOD-SCID); Severely immunocompromised mice obtained by crossbreeding knockout mice encoding the somatic y-chain gene. This mouse has defects in T, B, and NK cells and dysfunction of dendritic cells and macrophages. It is similar to NOD-SCID small Compared with mice, the survival time is longer, and the transplantation rate is higher, so it is a good PDX model mouse. Transplantation sites mainly include subcutaneous transplantation, orthotopic transplantation, subcapsular renal transplantation, and humanized xenograft models. There are many factors that affect the transplantation rate, which varies with different tumor types. It is necessary to carry out specific research on the PDX models of various tumors. [2]
How to make a PDX model?
The establishment of a PDX model relies on the direct transplantation of tumor specimens into immunocompromised animals. Mice with different immune deficiencies have different transplantation success rates (Nude < SCID < NOD/SCID < NSG), and the efficiency of PDX transplantation varies with the tumor. It varies by type, site of implantation, and tumor aggressiveness. This article mainly introduces three common PDX modeling parts and methods.
2.1 Subcutaneous PDX transplantation model
Subcutaneous transplantation using immunodeficient mice is currently the most commonly used transplantation method. This model provides heterogeneity of tumor cells, rarely metastasizes, and better simulates the initial tumor microenvironment. The tumor is implanted under the skin, and it is easy to observe and measure the growth of the tumor. The operation is relatively simple, and the technical difficulty is not high. For digestive system tumors, such as colon cancer, gastric cancer, and esophageal cancer, subcutaneous transplantation often has a higher success rate of PDX. However, for breast cancer, especially estrogen receptor-positive breast cancer, the success rate of transplantation is generally low, only 13%.
2.2 Renal subcapsular transplantation model
There are rich vascular structures under the renal capsule, which can provide sufficient nutrients, hormones, and oxygen to promote the growth of early tumor tissue and retain the heterogeneity and genetic characteristics of the primary tumor, which can greatly improve the success rate of tumor transplantation. It is known that transplanting human cervical cancer samples under the renal capsule can significantly increase the implantation rate of PDX models. For tumor implantation in the renal capsule, the implantation rate of non-small cell lung cancer is as high as 90%, while subcutaneous implantation is only 25%, high-risk endometrial cancer transplantation rate in the subrenal capsule was 62.5%, and subcutaneous transplantation was 50%. Furthermore, renal capsule implantation can greatly reduce tumor implantation time, which is one of the most important variables in the quest to realize real-time PDX data for personalized cancer therapy. Although subrenal capsule transplantation has a high transplant success rate, there are also some disadvantages. For example, transplantation at this site has high requirements for experimenters and requires extensive surgical experience. In addition, the size of the tumor is not easy to observe and measure.
2.3 Orthotopic allograft model
Most of the transplantation sites in PDX models are subcutaneous or renal capsules, lacking the in situ environment for tumor growth. The patient-derived orthotopic xenograft, PDOX model can generate metastasis, accurately simulate the natural environment of the primary tumor, and is usually used in the study of metastatic tumors. It has been found that transplanting tumor tissue into animal organs corresponding to the primary site can provide an in vivo environment suitable for tumor growth. Therefore, compared with the traditional PDX model, the PDOX model can more objectively and accurately simulate the evolution of human tumors in-vivo. The success rate of orthotopic transplantation of retinoblastoma can reach 70%, while the success rate of orthotopic transplantation of prostate cancer can reach up to 100%. [1]
What is the limitation of PDX model?
Although PDX models have significant advantages in preclinical cancer research, there are still some limitations that limit the wide application of PDX models.
First, the establishment of PDX models requires fresh tumor tissue, and the high cost of immunodeficient mice leads to high modeling costs, low success rate, and a long time for initial modeling. The time delay between the successful establishment of PDX models and the optimal treatment plan for patients has become a limiting factor in the implementation of personalized drug therapy.
Second, the success rate of tumor transplantation is not ideal, and only high-grade malignant tumors are suitable for PDX models.
Third, the conduct of PDX models requires a rigorous and time-consuming ethics approval process.
Fourth, PDX-derived tumor genomes change with passage number, which is not observed in the patient’s primary tumor.
Medicilon’s PDX Model
Now, Medicilon have the PDX models covering colon cancer,lung cancer,gastric cancer,breast cancer,liver cancer,pancreas cancer. Our research on PDX model includes molecular level genotyping and pharmacological efficacy evaluation service of orthotopic model, promising great prediction for clinical efficacy research.
[1]. ZHANG junhe, et al. Acta Laboratorium Animalis Scientia Sinica. Progress of PDX model application in oncology medicine. 2023,31(02)
[2].Jialiang Hu,et al. Pharmaceutical Biotechnology. PDX Model-Aided Cancer Disgnosis and Treatment. 2022,29(05),528-532 DOl:10.19526/j.cnki.1005-8915.20220517
[3]. Fan Liang, et al. China Biotechnology. Establishment and Application Progress of Patient-derived XenograftModel of Esophageal Cancer. 2022,42(08),74-84 DOI:10.13523/j.cb.2202036